
{kind=link}
Community Engagement Program Report
Oral Health Promotion through Community Leaders in Nagarparkar, Thar Pakistan
Executive Summary
This two-day outreach assessed oral health needs in Nagarparkar and co-designed a culturally anchored promotion program with local religious leaders. Key focus areas included dental caries, periodontal health, enamel defects, diet, hygiene practices, and betel nut (chalia) use. Engagement with Swamis/Pandits enabled skill transfer on toothbrushing demonstrations, basic dental screening, and motivational sessions for habit cessation.
Introduction
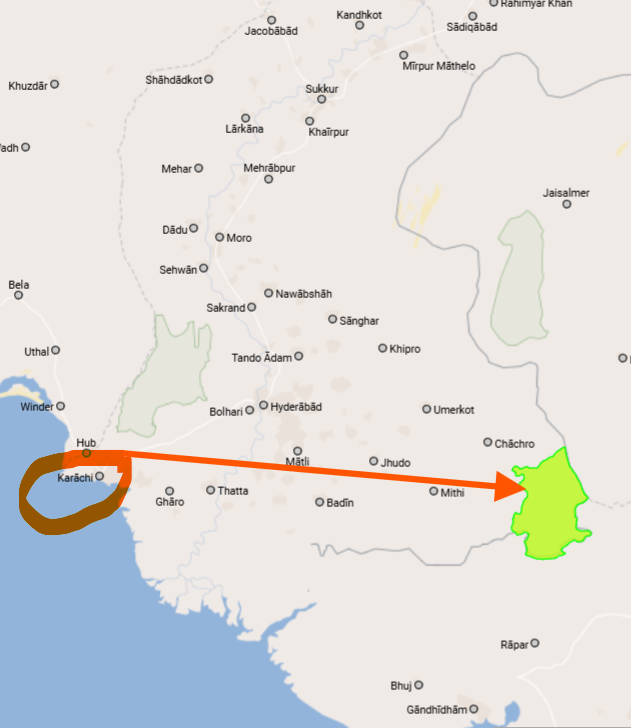
Nagarparkar lies in the Karoonjhar Mountain Range of Tharparkar District, Sindh, approximately 500 km from Karachi. The visit pursued two objectives: (a) assess the community’s oral health needs and baseline situation; (b) co-design an oral health promotion program with local leaders.
Demographics & Context
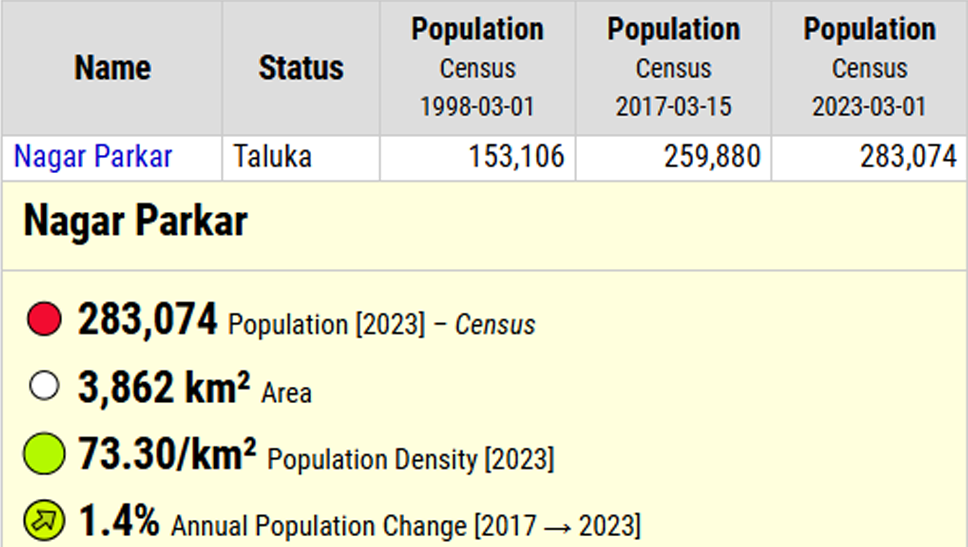
Population Trend
| Census Year | Population |
|---|---|
| 1998 | 153,106 |
| 2017 | 259,880 |
| 2023 | 283,074 |
Socio‑Cultural Notes
- Majority belongs to the Hindu Mehngwar community.
- Primary occupations include agriculture; diet relies on wheat and home‑grown vegetables.
- Oral hygiene commonly practiced with miswak (neem twig).
Visit Details
We visited Nagarparkar in the Karoonjhar Mountain Range located in the Tharparkar District which is approximately 500 km away from Karachi. It was a two-days visit (22 – 23 August, 2025) with two-folds objective: a) assess the oral health needs and baseline situation of the local community, and b) co-design oral health promotion program with the local community leader.
The need assessment included the assessment focusing the disease burden of dental caries, periodontal infections and dental / oral lesions, and the oral and social determinants such as dental hygiene, poor addictive habits and dietary practices. The enamel discoloration that initially appeared as fluorosis were found to hypoplastic changes which may be related to malnourishment. Attrition was also commonly observed related to betel nut consumption. Dental caries in at least 2 primary and one permanent tooth was observed in 2 out of every 10 persons in all age groups examined. Oral hygiene practices mostly included use of miswak (neem twig). Chalia (sweetened betel nut) was very frequently consumed by male adolescents and adults. The most frequent dietary habits included home grown vegetables and wheat with near to no intake of meat in any form.


Since the population consisted majority of Hindu (Mehngwar) community, their Mandir Swamis / Pandit were engaged to co-design oral health promotion program including oral hygiene and betelnut habit quit. One Pandit was approached who was taught the correct method of toothbrushing using single beaker rinse technique. The Pandit demonstrated toothbrushing to the Pujaris visiting the Mandir (Temple) followed by focus-group motivational session on betelnut quitting. He was taught to do dental screening using separate spoon (preferably plastic or wooden disposable) for each individual. Toothbrush kits were distributed by us to the individuals after screening. Follow-up visit will be done to assess the difference in the practices and betelnut consumption.


Needs Assessment Findings
- Dental caries observed in at least two primary and one permanent tooth in roughly 20% of individuals across age groups.
- Enamel defects resembling fluorosis were more consistent with hypoplastic changes, likely linked to malnutrition.
- Marked tooth wear/attrition associated with betel nut consumption.
- High prevalence of betel nut (chalia) use among male adolescents and adults.
- Diet pattern shows minimal to no meat intake; predominant intake of wheat and vegetables.
Intervention & Co‑Creation
Local religious leaders (Swamis/Pandits) were engaged to co-design and deliver oral health promotion:
- Toothbrushing Demonstration: Training on correct technique and the single‑beaker rinse method; live demonstrations to temple visitors.
- Habit Cessation: Focus‑group motivational session addressing betel nut use and oral health risks.
- Basic Screening: Guidance to conduct simple oral checks using separate disposable spoons for each individual.
- Resource Distribution: Toothbrush kits provided following screenings.
Follow‑Up Plan
- Monitor adoption of proper toothbrushing technique.
- Track reduction in betel nut consumption via brief community check‑ins.
- Train additional leaders to scale activities across neighborhoods.
Conclusion & Recommendations
- Leverage cultural leadership for sustained oral health promotion.
- Expand training cohorts; formalize refresher sessions every 3–6 months.
- Integrate dietary counseling and fluoride exposure guidance.
- Embed oral health modules in broader community health initiatives.
Credits & Acknowledgments
Prepared & submitted by Dr. Adnan Sukkurwala and Dr. M. Athar Khan. Supervision by Prof. Dr. Ambrina Qureshi.